
Average Cost to Build an Urgent Care Center in the USA (2026): Tenant Improvement vs. Ground-Up, and What You’ll Actually Pay by Region

The urgent care sector is one of the fastest-growing segments of healthcare real estate in the United States, and the construction pipeline is moving accordingly. According to Grand View Research, the U.S. urgent care market is projected to reach $75 billion by 2033, expanding at a compound annual growth rate of 9.8%. The number of urgent care centers nationwide nearly doubled between 2014 and 2023 — from 7,220 locations to more than 14,382 — and the buildout continues at pace, fueled by patient demand for walk-in access, ER diversion, and the expanding footprint of regional and national chains. Private equity has become a major driver of this expansion, with multi-site operators and health systems actively developing new locations across suburban and secondary markets.
For commercial real estate developers and healthcare operators planning new locations, one question comes up in almost every pre-development conversation: what is this going to cost to build? The problem is that "urgent care" encompasses an enormous range of facility types, scopes, and clinical configurations. A basic retail strip tenant improvement for a single-operator clinic in Tulsa bears almost no resemblance to a ground-up freestanding urgent care with CT imaging capability in suburban Boston. The per-square-foot figures circulating in the market are often stripped of that context — and they lead developers and operators into budgets that fall apart at the first GC pricing.
This article gives you the full picture: what urgent care construction actually costs in 2026, broken down by delivery method (tenant improvement vs. ground-up), clinical scope, and U.S. region. At Terrapin Construction Group, we build commercial medical and healthcare projects across all 50 states. The data here reflects current market conditions drawn from our own project experience, combined with publicly available benchmarks from RSMeans/Gordian, MedSpace USA, and published industry analyses.
The Urgent Care Construction Market in 2026
Demand fundamentals for urgent care construction are as strong as they have ever been. Emergency department overcrowding continues to push patients toward lower-cost, more accessible sites of care. RAND Corporation research estimates that roughly one-third of non-urgent ED encounters could be redirected to urgent care settings, representing more than $4 billion in annual savings to the healthcare system. U.S. enrollment in high-deductible health plans surpassed 64 million lives in 2024, incentivizing patients to price-shop and seek lower-cost care venues — a structural tailwind for urgent care operators that is not cyclical.
The supply-side picture is equally active. Hospital systems are embedding urgent care sites within integrated delivery networks as a throughput strategy. National chains including American Family Care and FastMed are pursuing acquisitions and new builds simultaneously. IBISWorld projects the urgent care market at $44.3 billion in 2026, with continued growth through the decade. In Denver alone, major health systems reported over $800 million in healthcare construction starts in 2025, much of it in outpatient and urgent care formats, according to The Denver Post's year-end construction review. The construction pipeline is real, active, and national.
On the cost side, 2026 is a more challenging environment than 2023 or 2024. MEP scopes — HVAC, electrical, and plumbing — have seen cost inflation of 15 to 25% compared to 2024 levels, according to MedSpace USA's February 2026 market report, which noted that medical office fit-out costs hit $412 per square foot nationally. Skilled labor shortages persist in virtually every major metro market, and electrical gear lead times for switchgear and transformers remain elevated. Developers and operators who entered contracts based on 2023 pricing assumptions are encountering budget shortfalls. Understanding current market pricing before committing to a site or a design is not optional — it is foundational.
Tenant Improvement vs. Ground-Up: Two Fundamentally Different Financial Propositions

The single most important variable in any urgent care construction cost conversation is the delivery path: are you doing a tenant improvement inside an existing commercial shell, or are you building from the ground up? These two paths operate in completely different cost universes and require completely different financial models.
Tenant Improvement (TI) Build-Out
A tenant improvement is a build-out from an existing commercial shell — typically a vacant retail, office, or second-generation medical space. You are working inside a building that already exists: the structure, roof, and building envelope are already in place. Your construction scope is the interior: partition walls, plumbing, electrical upgrades, HVAC distribution, flooring, ceilings, cabinetry, and all the specialized clinical infrastructure an urgent care requires. For urgent care specifically, that clinical infrastructure is significantly more complex than standard commercial office work, which is why the per-square-foot cost is considerably higher than a standard office TI.
The cost advantage of a TI over ground-up is real and significant: you are not paying for land, site work, foundation, structure, or building envelope. The cost disadvantage is that you are inheriting whatever the existing building gives you — ceiling heights, column spacing, structural loads, available electrical service, and existing MEP infrastructure — and your clinical layout must work within those constraints. A vanilla shell with 14-foot ceilings, adequate electrical service at the panel, and a ground-floor location with accessible parking is a fundamentally different TI starting point than a second-floor retail suite in a 1980s strip center with 9-foot ceilings and undersized electrical service.
One financial lever that makes TI projects more attractive for urgent care operators than they initially appear is the tenant improvement allowance. Because urgent care build-outs include significant plumbing, heavy electrical upgrades, and HVAC work that permanently improves the value of the landlord's property, landlords in most markets are motivated to contribute toward build-out costs. In competitive medical office markets, TI allowances of $50 to $100 per square foot are negotiable and represent a material offset to out-of-pocket capital requirements.

Ground-Up Construction
A ground-up urgent care build is a complete new construction project: site selection and control, civil engineering and site work, foundation, structure, building envelope, MEP, and full interior clinical buildout. Every decision is yours to make — ceiling heights, structural bays, electrical service size, parking and patient flow configuration, and site accessibility. You are not constrained by an inherited building, but you are taking on the full cost stack of new construction.
Ground-up projects require more capital, longer timelines, and more complexity than TI work, but they deliver a clinical facility that is purpose-built for the operator's specific workflow and patient volume requirements. For regional chains and multi-site operators establishing a branded prototype, ground-up is often the right choice. For first-time operators or smaller operators in cost-sensitive markets, a TI in the right shell space may deliver better unit economics.
TCG provides preconstruction services, commercial general contracting, construction management, and design-build delivery for both TI and ground-up healthcare projects. The earlier a GC is engaged in the process, the more value is available to capture — on cost certainty, timeline, and design coordination.
Why Urgent Care Construction Costs More Than Standard Commercial Office Space

The per-square-foot cost of an urgent care build-out is materially higher than a standard commercial office TI of the same size. Understanding why requires understanding what an urgent care actually contains that a conventional office does not.
Medical-Grade HVAC and Ventilation
Urgent care HVAC must comply with ASHRAE Standard 170, Ventilation of Health Care Facilities, which mandates a minimum of six air changes per hour in exam rooms and 15 air changes per hour in procedure rooms. The infection control requirements for an urgent care — which sees patients with respiratory illness, open wounds, and communicable conditions daily — demand medical-grade ventilation design that standard commercial HVAC systems cannot deliver. Healthcare-grade HVAC systems, which include dedicated exhaust from exam and procedure rooms, negative pressure capability in isolation spaces, and HEPA filtration in clinical zones, represent one of the most significant cost premiums in an urgent care build-out over standard commercial construction. Per Maxx Builders' 2026 Texas medical office cost analysis, MEP scopes for healthcare facilities run 15 to 25% above standard commercial levels and show the most persistent inflation of any construction category.
X-Ray Suite with Radiation Shielding
Approximately 75% of urgent care centers offer on-site digital X-ray services, according to market data from the Urgent Care Association. An X-ray room is not a standard clinical room with better lighting. It requires lead-lined drywall or lead-backed panels on all primary and secondary barrier walls, a shielded control position with a leaded glass window, lead-lined door assemblies, and dedicated HVAC. According to PrizMed Imaging's buildout cost guide, a basic X-ray room buildout costs between $40,000 and $120,000 depending on scope, equipment type, and local requirements. The lead shielding component alone runs $15,000 to $35,000 for a standard single-room suite, per detailed shielding cost breakdowns published by metal-buildings.org. A qualified medical physicist must review the shielding design and certify adequacy before the state will issue an imaging equipment license — a non-negotiable construction step that first-time urgent care builders routinely underbudget.
Plumbing Density and Medical Gas
Each exam room in an urgent care requires at least one plumbing fixture — a hand sink at minimum, with procedural sinks where minor surgical procedures are performed. For a 3,500-square-foot urgent care with seven or eight exam rooms, you are installing plumbing rough-in for eight to twelve fixtures in a space where a standard commercial office of the same size might have two or three restroom fixtures total. If the operator includes oxygen therapy, a piped medical gas system adds another $10,000 to $30,000 to the construction scope, depending on the number of outlets. The aggregate plumbing density of an urgent care build is several multiples of a standard commercial office TI of equal square footage.
ADA Compliance and Patient Flow Infrastructure
All urgent care facilities must meet ADA Standards for Accessible Design, including accessible exam room clearances, accessible restrooms, widened corridors to accommodate mobility devices, and accessible reception counters. The patient flow configuration of an urgent care — separate clean and dirty corridors in higher-acuity facilities, registration and triage areas, waiting rooms designed for sick and well patient separation, and staff workstation visibility to the waiting area — creates a level of floor plan complexity that drives custom framing, millwork, and build-out cost above standard commercial benchmarks.
Technology and Low-Voltage Infrastructure
A competitive urgent care facility in 2026 requires structured cabling and data ports at every clinical workstation, integration with an electronic health record system, HIPAA-compliant network architecture, digital X-ray PACS integration, point-of-care lab instrumentation, and increasingly, telehealth-capable consultation rooms. According to the American Medical Association's practice management resources, patient flow technology and digital intake systems have become table-stakes infrastructure for urgent care operators competing in mature markets. The low-voltage scope of a properly built urgent care facility adds $15,000 to $40,000 to the construction budget over a standard commercial office TI.
Typical Urgent Care Footprints: What You're Actually Building

Before getting into per-square-foot costs, it is worth establishing what a typical urgent care build actually encompasses in terms of footprint and scope. There is no single "standard" urgent care prototype, but the following configurations represent the most common buildout profiles in the current market.
Small-Format Urgent Care: 1,500–2,500 Square Feet
A compact urgent care in this footprint typically accommodates four to six exam rooms, a triage and registration area, one restroom, and a small waiting area. It may or may not include on-site X-ray capability. This format is common in urban retail sites and strip center in-line spaces where real estate constraints limit the footprint. It represents the highest clinical density per square foot and the most compressed patient flow of the common formats. Clinical efficiency suffers relative to larger formats, but capital requirements are lower.
Mid-Size Urgent Care: 2,500–4,000 Square Feet
This is the most common configuration for new urgent care builds, particularly for franchise operators and health system-affiliated sites. A 3,500-square-foot urgent care typically accommodates seven to eight exam rooms, a dedicated triage room, an X-ray suite, a lab draw station, a procedure room for minor surgical work (laceration repair, splinting, I&D), a waiting area sized for 10 to 15 patients, two restrooms, and administrative and staff space. This is the "standard" prototype that most cost benchmarks in the market are built around.
Large-Format Urgent Care or Urgent Care with Advanced Imaging: 4,000–7,000 Square Feet
Larger urgent care builds — particularly those with CT capability, occupational health services, or physical therapy adjacency — require 4,000 to 7,000 square feet or more. CT rooms require more extensive radiation shielding than standard X-ray suites, reinforced structural slabs for equipment weight, and dedicated HVAC for imaging equipment heat loads. The clinical differentiation of large-format urgent cares also increasingly includes observation beds and extended-stay capability, which further expand the footprint and MEP complexity. According to the Urgent Care Association's market data, advanced diagnostic capability is a major competitive differentiator in saturated markets and is driving larger prototypes in health-system-affiliated urgent care networks.
Urgent Care Construction Cost Per Square Foot: 2026 National Benchmarks

The following ranges represent current national average hard construction costs. They exclude land acquisition (for ground-up), architectural and engineering fees (typically 8 to 12% of hard costs), permitting, owner-supplied medical equipment, IT hardware, and pre-opening operating expenses. Regional adjustments are addressed in the following section.
Tenant Improvement: Basic Clinical Renovation
A basic urgent care TI from a commercial shell — partition walls, flooring, ceilings, standard commercial HVAC distribution upgrades, code-minimum electrical, and modest plumbing for exam room sinks and restrooms, without X-ray capability — runs $150 to $225 per square foot at national average labor rates in open-shop markets. This is the floor-level entry point for urgent care construction. The per-square-foot figure looks modest, but the absence of X-ray infrastructure materially limits the clinical scope and competitive positioning of the resulting facility in most markets.
Tenant Improvement: Full-Scope Urgent Care with X-Ray
A full-scope urgent care TI — medical-grade HVAC meeting ASHRAE 170 requirements, healthcare-grade electrical distribution, exam room plumbing density, X-ray suite with lead shielding, ADA-compliant clinical layout, structured cabling, and quality interior finishes — runs $225 to $350 per square foot at national averages in competitive open-shop markets. This is the cost range most operators building a functional, competitive urgent care in a mid-cost U.S. market should be planning against. Per Arrant Construction's 2026 medical construction cost guide, standard medical office buildings and urgent care centers sit at $400 to $600 per square foot for full-scope construction, with the lower end of that range reflecting efficient open-shop markets and standard finishes.
Tenant Improvement: Premium Markets or Complex Clinical Scope
In high-cost coastal markets, or for urgent care builds with CT imaging capability, advanced procedural rooms, or premium brand standards, TI construction costs run $350 to $500 or more per square foot. MedSpace USA reported medical office fit-out hitting $412 per square foot nationally in February 2026, with coastal urban markets pushing well above that level. Autodesk's commercial construction cost benchmarks confirm medical office buildings averaging around $498 per square foot, with specialty clinics reaching $619 per square foot. These figures reflect the full cost of medical-grade construction in major metro markets and are a meaningful reference point for owners evaluating high-cost-market TI projects.
Ground-Up Construction: Freestanding Urgent Care
A freestanding ground-up urgent care — including site work, foundation, structure, building envelope, and full clinical interior buildout — runs $300 to $600 per square foot at national average construction costs. The range is wide because site conditions, structural system selection, and clinical scope vary significantly between projects. Claris Design•Build's 2026 medical office construction benchmarks place medical office buildings at $375 to $1,018 per square foot for ground-up construction, with location, design complexity, and the integration of specialized medical systems driving the range. For a typical 3,500-square-foot urgent care, the all-in project cost excluding land runs $700,000 to $2,000,000 or more depending on market, site conditions, and clinical scope.
Pre-engineered metal building systems offer a meaningful structural cost reduction for ground-up urgent care projects, particularly in suburban and semi-rural markets where architectural constraints are less restrictive. TCG evaluates PEMB suitability as part of preconstruction for every applicable ground-up project. The structural cost savings of 15 to 25% compared to conventional light-frame construction can be redirected into higher clinical infrastructure spend — better HVAC, more imaging capability, or enhanced finishes — without increasing the total project budget.
Regional Construction Cost Breakdown: What You'll Actually Pay by Market

National averages are a useful orientation point, but they are not what you will pay in your specific market. Commercial construction costs vary 25 to 40% above national averages in major coastal metro markets, while Southern and Mountain West markets frequently price at or below the national average. Here is how those differences break down across the five major U.S. construction cost regions, with project-level cost implications for a standard 3,500-square-foot full-scope urgent care build.
Southeast and South-Central (TX, FL, GA, TN, NC, SC, AL, MS, AR, OK)
The Southeast represents the most favorable construction cost environment for urgent care development in the United States. Right-to-work states, competitive subcontractor markets, and lower union density keep labor costs 10 to 20% below national averages. A full-scope urgent care TI in Dallas, Houston, Atlanta, Nashville, or Charlotte runs approximately $175 to $275 per square foot in hard construction costs. Terrapin's Houston office actively builds medical and commercial projects across the Texas market, where we see competitive pricing from a deep subcontractor base and generally faster permit timelines than coastal markets. A typical 3,500-square-foot TI urgent care in this region runs $600,000 to $960,000 all-in, including soft costs but excluding land and medical equipment. Ground-up construction for the same footprint runs $700,000 to $1,200,000 all-in excluding land.
Texas in particular is an active market for urgent care development. Major health systems, regional chains, and independent operators are all expanding in Texas metros. Maxx Builders' 2026 Texas medical construction analysis notes that design-build delivery can reduce change orders by approximately 10 to 15% and compress project schedules by up to 30% in the Texas market — advantages that compound over multiple locations for multi-site operators.
Midwest (IL, OH, IN, MI, MN, WI, MO, IA, KS, NE)
The Midwest tracks closely to national average construction costs with important urban exceptions. Chicago is a union-heavy market that adds 15 to 25% to labor costs relative to downstate Illinois or neighboring Indiana. Secondary and tertiary Midwest markets — Columbus, Indianapolis, Kansas City, Des Moines, Omaha — price at or near the national average with a reliable skilled trades workforce. A full-scope TI urgent care in most Midwest secondary markets runs $175 to $280 per square foot. For a 3,500-square-foot urgent care, that produces a TI total of $610,000 to $980,000 all-in including soft costs. Ground-up in these markets runs $750,000 to $1,350,000.
The U.S. Bureau of Labor Statistics Producer Price Index for healthcare building construction tracks construction cost escalation across all four U.S. census regions and provides the most rigorous regional cost data available. The BLS data consistently shows the Midwest tracking at or near the national average while the Northeast and West maintain persistent premiums.
Mountain West and Southwest (CO, UT, WY, ID, MT, NV, AZ, NM)
The Mountain West has seen significant construction cost appreciation driven by population growth, strong commercial development activity, and a skilled labor market that is not keeping pace with demand. Colorado, Utah, Idaho, and Arizona in particular are active urgent care markets. Construction costs in Denver, Salt Lake City, Boise, and Phoenix run 10 to 20% above the national average for healthcare work. Terrapin's Denver and Sheridan offices build across this region. A full-scope TI urgent care in Colorado or Utah runs $200 to $325 per square foot, producing an all-in 3,500-square-foot TI total of $700,000 to $1,140,000. Ground-up in this region runs $850,000 to $1,500,000.
Northeast (NY, NJ, MA, CT, PA, MD, DC, VA)
The Northeast is the most expensive construction region in the United States for urgent care development. Union labor in most major markets, high permit fees, dense urban sites that limit parking and patient flow configuration, and stringent local code requirements all contribute to premiums of 30 to 50% above the national average. Terrapin's Albany office serves the greater Northeast market. Full-scope TI urgent care construction in the New York, Boston, Philadelphia, and Washington D.C. markets runs $275 to $450 per square foot. An NYC-area urgent care TI of 3,500 square feet can reach $1,000,000 to $1,575,000 all-in including soft costs. Ground-up freestanding urgent care in the Northeast, where land and site work costs are already elevated, runs $1,100,000 to $2,000,000 or more for a standard footprint.
The revenue-side offset is real: reimbursement rates and patient volume in the Northeast are among the highest nationally, with revenue per patient visit running 20 to 30% above the national average in many markets. The unit economics still work — but the capital requirement is higher, and budget errors are more consequential.
West Coast (CA, WA, OR)
California is the highest absolute cost construction environment in the country for urgent care development. High labor costs (both union and prevailing wage requirements), California's Office of Statewide Health Planning and Development (OSHPD/HCAI) oversight for healthcare facilities, Title 24 energy code requirements, CEQA environmental review in many jurisdictions, and seismic engineering requirements for structural systems all drive construction costs significantly above the national average. A full-scope TI urgent care in the Los Angeles Basin, Bay Area, or San Diego runs $300 to $475 per square foot. Ground-up freestanding urgent care in California major metros: $1,000,000 to $2,200,000 or more for a 3,500 SF facility, excluding land.
Oregon and Washington, outside of the Portland and Seattle metros, are somewhat more accessible — roughly 20 to 30% above the national average in most secondary markets. Seattle carries union premiums approaching Northeast levels. Portland has at times ranked among the most expensive U.S. cities for commercial construction on a per-square-foot basis, according to EB3 Construction's regional cost analysis.
Key Considerations for Urgent Care Construction: What Moves the Number Most

Within any format and region, these are the variables that create the greatest cost variance between projects at the low end and the high end of the range. Most of them are decisions made before construction starts, which is why early GC involvement through preconstruction services is the single most valuable investment an urgent care developer or operator can make in the pre-development phase.
1. Shell Condition and Second-Generation Space
The condition of the base building fundamentally changes the TI cost equation. A true vanilla shell — an unimproved retail or medical office space with concrete floors, exposed ceilings, and utilities stubbed to the space — requires more construction work than a second-generation medical space that already has clinical-grade plumbing, electrical distribution, and exam room partitions in place from a prior occupant. Second-generation urgent care or medical office spaces represent the most capital-efficient starting point for a TI project. Conversely, a second-generation space configured for a completely different clinical use may require full demolition before a new urgent care can be built, eroding the cost advantage. Experienced owners' representatives assess base building condition and demolition scope during site due diligence before lease execution.
2. Imaging Scope: X-Ray Only vs. CT Capability
The decision to include CT imaging capability is the single largest cost driver within urgent care clinical scope. A standard single-room digital X-ray suite adds $40,000 to $120,000 to the construction budget, including lead shielding. A CT room requires substantially heavier radiation shielding, a reinforced structural slab to bear the weight of the scanner, dedicated HVAC for equipment heat loads, and additional electrical service for the scanner's power draw. A CT suite addition can add $200,000 to $400,000 or more to the construction budget above an X-ray-only build. For operators who have not finalized their imaging strategy before construction starts, this is a scope change that invalidates the original budget and schedule.
3. Union vs. Open-Shop Labor Market
The geographic distribution of union labor creates a structural cost difference that is not within an operator's control. Union-heavy markets — New York, Boston, Chicago, Philadelphia, Seattle, and most of California — carry labor premiums of 20 to 35% over open-shop markets in the South and Mountain West. The AGC's Construction Inflation Alert tracks these labor market differentials and confirms their persistence. This does not mean open-shop is universally better — union markets often have superior productivity on complex MEP-intensive healthcare projects where coordination and quality control are critical. But it is a real cost variable that must be incorporated into any market-to-market budget comparison.
4. Site Conditions for Ground-Up Projects
For ground-up urgent care development, site conditions are the most underestimated cost driver. A fully improved outparcel on a commercial corridor with existing utilities, flat topography, and no environmental issues is a fundamentally different proposition than a raw parcel requiring utility extensions, grading, storm water management, and environmental remediation. The difference in site work costs alone can be $150,000 to $400,000 on the same building footprint. Thorough site due diligence by an experienced GC or owners' representative before entering into a purchase agreement is not optional on ground-up medical projects.
5. Material Costs and Tariff Exposure in 2026
As we've addressed in detail elsewhere, current Section 232 tariffs on steel, aluminum, and copper are running at 50% and are embedded in every commercial and healthcare build through structural framing, MEP rough-in, and electrical service. Urgent care builds are particularly exposed because of MEP density — the copper content of a healthcare-grade electrical and plumbing rough-in is multiples of a standard commercial build on the same footprint. Operators who front-load materials procurement through a GC with established supply chain relationships can meaningfully reduce mid-project price exposure.
6. Regulatory Timeline and Permitting Complexity
Urgent care construction triggers healthcare occupancy classification review — typically a Business (B) occupancy for clinics treating ambulatory patients — which requires more rigorous plan review, fire marshal inspection, and ADA compliance verification than standard commercial permits. In California, HCAI review adds additional layers of state-level approval. Some jurisdictions require certificate of need (CON) review for new healthcare facilities. Budget $10,000 to $30,000 for permit fees depending on market and project size, and — more importantly — build healthcare-realistic permit timelines into project scheduling. A 60- to 90-day permit window in a cooperative jurisdiction can extend to 120 to 180 days in a complex municipal or state-review market.
7. Equipment Lead Times and Procurement Sequencing
Digital X-ray systems run $75,000 to $200,000 in equipment cost alone, and CT scanners represent capital commitments of $400,000 to $1,500,000. Both have lead times that, when not managed correctly, delay clinical openings by months. More consequentially, equipment dimensions, utility requirements, and structural loading specifications must be coordinated with the GC before walls are framed and MEP rough-in begins. TCG's equipment procurement division helps operators get long-lead clinical equipment on order at the right point in the project sequence, coordinating with rough-in and utility installation so equipment arrivals align with construction readiness.
The Four Planning Mistakes That Blow Urgent Care Budgets
After managing medical and commercial construction projects across the country, these are the four most consistent planning failures that derail urgent care builds.
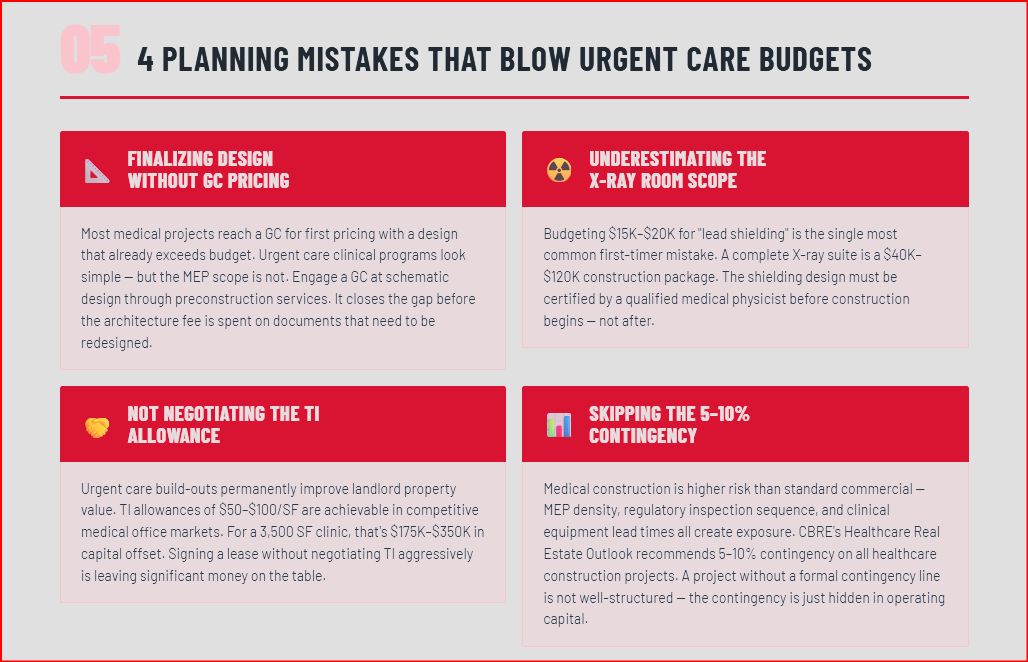
Finalizing Design Without GC Pricing
According to industry benchmarks from the American Institute of Architects, the majority of commercial and medical projects are delivered to a GC for first pricing with a design that already exceeds the owner's budget. Urgent care projects are especially vulnerable to this pattern because the clinical program looks straightforward on paper — exam rooms, a waiting area, X-ray suite — but the MEP scope required to build it correctly is anything but simple. Healthcare architects working without real-time cost data consistently underestimate medical-grade HVAC scope, plumbing density, and the cost implications of ASHRAE 170 compliance. Engaging a GC at schematic design through preconstruction services closes the gap between design intent and buildable reality before the architecture fee is spent on a set of documents that needs to be redesigned.
Underestimating the X-Ray Room Scope
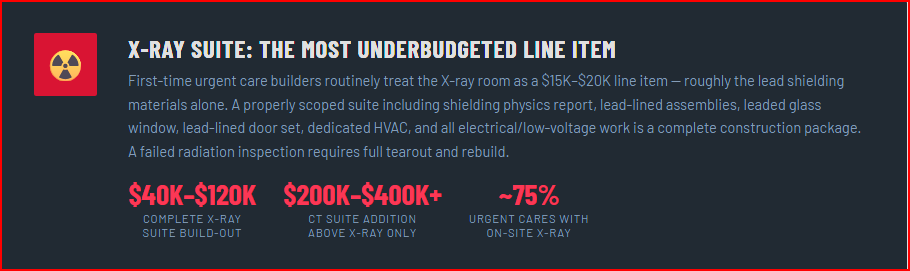
Operators and developers new to healthcare construction frequently treat the X-ray room as a modest line item. A properly scoped X-ray suite — including the shielding physics report, lead-lined assemblies, leaded glass observation window, lead-lined door set, dedicated HVAC for the control position, and all associated electrical and low-voltage work — costs $40,000 to $120,000 as a complete construction package, per PrizMed Imaging's comprehensive buildout cost guide. A failed radiation shielding inspection requires tearout and rebuild, and delays the state imaging equipment license. The shielding design must be reviewed by a qualified medical physicist before construction begins.
Not Negotiating the Tenant Improvement Allowance
Medical build-outs involve significant plumbing, heavy electrical upgrades, and HVAC work that permanently improves the value of the landlord's property. In most commercial real estate markets, landlords are motivated to offer meaningful TI allowances for medical tenants precisely because of this. In competitive medical office markets, TI allowances of $50 to $100 per square foot are achievable. For a 3,500-square-foot urgent care, that represents $175,000 to $350,000 in capital offset — enough to materially change project feasibility. Operators who sign leases without negotiating TI aggressively are leaving significant capital on the table. TCG's team works closely with operators' brokers and their architects to ensure TI scope is well-documented and that construction budgets reflect what the allowance will and will not cover.
Ignoring the 5–10% Contingency Requirement
Medical construction is inherently higher risk than standard commercial construction because of the density and complexity of MEP systems, the regulatory inspection sequence, and the lead times on clinical equipment. A project that reaches bidding or GMP pricing without a formal contingency line in the budget is not a well-structured project — it is a project whose contingency is hidden in the owner's operating capital. CBRE's Healthcare Real Estate Outlook consistently recommends 5 to 10% contingency on healthcare construction projects given sustained labor market and materials pricing volatility. Budget a formal contingency. It will be used.
Why Design-Build Delivery Creates Specific Value for Urgent Care Projects
Of all the clinical build types in healthcare construction, urgent care is among the formats where design-build delivery creates the most measurable value for owners. The reasons are structural.
Urgent care clinical programs have well-defined room-type requirements that repeat across locations for multi-site operators. Modular, standardized exam room layouts reduce custom millwork costs, simplify MEP rough-in, and accelerate construction timelines without clinical compromise. When a GC is integrated at the design stage, the structural system, MEP distribution, and finish specifications can be value-engineered in real time against current market pricing — not estimated from historical data by an architect working independently. Maxx Builders' 2026 analysis documents design-build savings of 10 to 15% on change orders and schedule compression of up to 30% compared to traditional design-bid-build procurement in the Texas medical market.
For multi-site urgent care operators establishing a prototype, the design-build advantage compounds over locations. A standardized prototype that has been value-engineered once — structural system, MEP design, finish specifications, equipment coordination sequence — delivers faster and cheaper on every subsequent build. TCG's preconstruction team works with operators and their architects to develop exactly this kind of standardized, cost-validated prototype that travels across markets.
Financing an Urgent Care Build-Out
Most new urgent care operators and developers finance construction through a combination of vehicles. SBA 7(a) and 504 loans are commonly used for medical facility construction and offer favorable terms with lower down payment requirements than conventional commercial loans. Conventional commercial real estate loans are appropriate for ground-up builds where the land is being purchased. Equipment financing for digital X-ray systems, CT scanners, and point-of-care lab equipment is available from clinical equipment vendors including Patterson Companies and Henry Schein, as well as from healthcare-focused commercial lenders. For acquisitions of existing urgent care operations requiring renovation, practice acquisition loan programs are available through multiple healthcare lending specialists.
When modeling project financing, it is important to separate the construction loan from the equipment financing and to ensure that the construction draw schedule is aligned with the GC's payment milestones. A mismatch between financing availability and GC payment obligations is a common source of project delays on medical builds. Engaging a construction manager or owners' representative who understands medical project financing can prevent this misalignment.
Start Your Urgent Care Project the Right Way
The difference between an urgent care project that delivers on its pro forma and one that doesn't almost always traces back to decisions made in the first 60 days of the development process — site selection, format definition, GC engagement, and budget validation. That's the window where the most value is created and the most money is saved.
Terrapin Construction Group provides preconstruction services, commercial general contracting, construction management, and design-build delivery for urgent care and medical office projects nationwide. If you're planning an urgent care build and want a frank, current-market conversation about what it's going to cost to build, we'd welcome a 30-minute call.
Schedule a conversation → calendly.com/will-terrapincg/30min
You may also find the following related reading useful:
Sources
Grand View Research — U.S. Urgent Care Centers Market Analysis
Grand View Research — U.S. Urgent Care Centers Market Report (2025–2030)
Maxx Builders — Medical Office Construction Costs Texas 2026
Arrant Construction — Medical Construction Costs Complete Guide
Claris Design•Build — Commercial Construction Cost Per Square Foot 2025 Update
metal-buildings.org — Urgent Care Construction Cost: Full Breakdown 2026
HomeGuide — Commercial Construction Cost Per Square Foot, 2026
BLS — Producer Price Index for Healthcare Building Construction
Last updated: March 2026. Cost data is directional and based on publicly available industry benchmarks. Actual costs will vary by project scope, location, contractor, and market conditions. Consult a qualified contractor and healthcare architect for project-specific estimates.
Frequently Asked Questions: Urgent Care Construction Costs
How much does it cost to build an urgent care center per square foot?
Building a ground-up urgent care center costs $200 to $600 per square foot, or $600,000 to over $2 million all-in for a typical 3,500-square-foot facility. TI buildout in existing shell space runs $120 to $350 per square foot. Cost depends heavily on imaging scope — a basic urgent care with exam rooms costs far less than a facility with X-ray, CT, or MRI suites.
How much do imaging suites add to urgent care construction costs?
Adding diagnostic imaging — X-ray, CT, or MRI — can increase total construction cost by 20–35%. Imaging suites require radiation shielding, reinforced floor slabs, dedicated electrical circuits, specialized HVAC, and equipment-specific room dimensions. Equipment alone can cost $150,000 to $1.5 million depending on modality.
What is the difference between freestanding and in-line urgent care construction costs?
Freestanding ground-up urgent care costs $200–$600/SF all-in including site work, building, and MEP. In-line TI buildout in a strip center or retail shell costs $120–$350/SF but avoids land and site work costs. Freestanding facilities offer better visibility and signage, while in-line locations offer lower upfront investment and faster time to open.
How long does it take to build an urgent care center?
TI buildout: 3–5 months. Ground-up freestanding: 6–10 months. Complex builds with imaging suites in high-regulation markets: 8–12+ months. Medical equipment lead times must be coordinated with rough-in to avoid schedule delays.
How do urgent care construction costs vary by region?
Southeast markets (Houston, Atlanta, Charlotte) run 10–20% below national average. Midwest near average. Mountain West (Denver) 10–20% above. Northeast and West Coast 25–50% above. Union labor requirements in the Northeast are a significant cost driver for healthcare construction.
How do I get an urgent care construction estimate?
TCG's AI construction estimator provides preliminary urgent care cost estimates. Schedule a call for formal preconstruction budgeting.